Carotid endarterectomy
Definition
Carotid endarterectomy (CEA) is a surgical procedure that is performed to remove deposits of fat, called plaque, from the carotid arteries in the neck. These two main arteries, one on each side of the neck, deliver blood and oxygen to the brain. Plaque builds up in large- and medium-sized arteries as people get older, more in some people than others depending on lifestyle and hereditary factors. This build up is a vascular disease called atherosclerosis, or hardening of the arteries. When this happens in either one or both of the carotid arteries, they can become narrowed, a condition called stenosis. During a carotid endarterectomy, a surgeon removes the fatty deposits to correct the narrowing and to allow blood and oxygen to flow freely to the brain.
Purpose
Carotid endarterectomy is a protective procedure intended to reduce the risk of stroke, a vascular condition also known as a cardiovascular accident (CVA). In studies conducted by the National Institute of Neurological Disorders and Stroke (NINDS), endarterectomy has proven to be especially protective for people who have already had a stroke, and for people who are at high risk for stroke or who have already been diagnosed with significant stenosis (between 50% and 70% blockage).
Demographics
The National Stroke Association reports that twothirds of stroke victims are over age 65. Risk is shown to double with each 10 years over age 55. Men are more at risk than women, although most stroke survivors over age 65 are women, which may be partly because there are more women than men in this age group. African Americans have been shown to be at greater risk for stroke than other racial groups in the United States. Risk is also higher in people who have a family history of stroke as well as people with diabetes, because of the circulatory problems associated with diabetes. People with high blood pressure, also called hypertension, have four to six times the risk of stroke.
Nearly 700,000 strokes occur in the United States each year, with about 150,000 deaths, making stroke the third leading cause of death behind heart disease and cancer. Stroke is also responsible for the high number of disabled adults in the United States; two million stroke survivors have some permanent disability. The annual cost to the country for treating stroke and disabilities caused by stroke is about $40 billion.
Description
The presence of fatty deposits in the carotid arteries of the neck is the most significant risk factor for ischemic stroke, which represents 80% of all strokes. A stroke can be either ischemic, which is an interruption of blood flow in a narrowed carotid artery, or hemorrhagic, which involves bleeding in the brain. Carotid endarterectomy is performed as prevention of ischemic strokes.
Some people at high risk for ischemic stroke have disturbing symptoms that can occur periodically and last from minutes to up to 24 hours, and then disappear. These episodes are called transient ischemic attacks (TIA). The symptoms are the same as actual stroke symptoms. The symptoms of TIA and ischemic stroke may include:
- Numbness, muscle weakness, or paralysis of the face, arm, or leg, usually on one side of the body, and usually occurring suddenly.
- speech or vision difficulties
- sudden loss of understanding, confusion
- lightheadedness or fainting spells
- loss of balance with difficulty walking and moving; poor coordination
- severe headache with no obvious cause, either sudden or persistent
About 35% of people who have TIAs will have a stroke within five years. The risk of stroke goes up with age and is greatest in people whose blood pressure is higher than normal. High blood pressure stresses the walls of blood vessels, particularly when the vessels are blocked with plaque and so space for blood to pass is reduced.
Carotid endarterectomy has been performed since the 1950s as a stroke-prevention method. During the 1990s, about 130,000 carotid endarterectomies were performed each year in the United States. Because the surgery itself presents a high risk of complications, surgeons will look at the possible benefits and risks for each patient and compare them with such medical treatment as drug therapy to reduce plaque, cholesterol, and blood pressure. Carotid endarterectomy is typically performed on those who will benefit most from the surgery and who have the lowest risk for postoperative complications. Good candidates include:
- People who have already had one or more TIA episodes in a six-month period, with 70% narrowing of the carotid arteries supplying the part of the brain affected by the TIA.
- People who have had a mild stroke in the past six months but who are not significantly disabled and whose carotid arteries are at least 70% narrowed.
- People who have not had a stroke or TIA, but their carotid arteries are narrowed 60% or more and they have low risk of complication from having the surgery.
Carotid endarterectomy is not recommended for:
- People whose risk of complications from the surgery is greater than the intended benefits. The presence of other problems such as heart disease may increase risk.
- People who have had a TIA but their carotid arteries are less than 50% narrowed.
- People who have had a stroke or TIA because arteries other than the carotid arteries are blocked.
- People whose carotid arteries are blocked above a point on the neck where they can be reached easily during surgery.
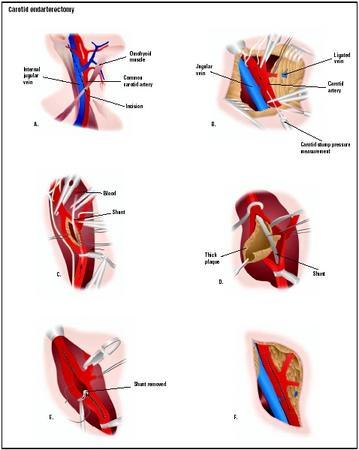
The endarterectomy procedure takes about an hour to perform. General anesthesia is usually administered. A vascular surgeon or neurosurgeon will usually perform the surgery. During the procedure, a small incision is made in the neck below the jaw to expose the carotid artery. Blood that normally flows through the artery must be diverted in order to perform the surgery. This is accomplished by rerouting the blood through a tube (shunt) connecting the vessels below and above the surgical site. The carotid artery is opened and the waxy fat deposit is removed, sometimes in one piece. If the carotid artery is observed to be too narrow or too damaged to perform the critical job of delivering blood to the brain, a graft using a vein from the patient's leg may be created and stitched (grafted) onto the artery to enlarge or repair it. The shunt is then removed, and incisions in the blood vessels, the carotid artery, and the skin are closed.
Diagnosis/Preparation
Diagnosis
The presence and degree of stenosis in the carotid artery must be determined before a doctor decides that carotid endarterectomy is necessary. Carotid stenosis can sometimes be detected in a routine checkup, especially when a detailed history reveals to the doctor that the patient has experienced symptoms of TIA or stroke. The doctor will use a stethoscope to listen to blood flow in the carotid artery and may hear an abnormal rushing sound called a "bruit" (pronounced "brew-ee") that will indicate narrowing in the artery. The absence of sound, however, does not mean there is no risk. More extensive testing will most likely have to be done to determine the degree of stenosis and the potential of risk for the patient. These tests may include:
- Ultrasound imaging with Doppler—a painless, noninvasive imaging test that measures sound waves directed into the body and returned to the ultrasound machine as echoes. Usually these echoes are visualized as an image on a screen; Doppler captures the sound as the echoes bounce off of moving blood in the carotid artery, giving some indication of the amount of blockage as the ultrasound probe moves up and down the arteries on each side of the neck.
- Computed tomography (CT) or computer-assisted tomography (CAT scan)—a series of cross-sectional x rays of the head and brain that can rule out other causes for the symptoms but cannot detect carotid artery stenosis.
- Oculoplethysmography (OPG)—a procedure that measures the pulsing of arteries behind the eye, which can show carotid artery blockage.
- Arteriography and digital subtraction angiography (DSA)—special x-ray procedures using dye in the patient's vascular system. These tests are invasive and can actually cause a stroke, but they do indicate more exactly what degree of stenosis is present. The doctor will have to weigh the extent of risk and how much the patient will benefit from the tests.
- Magnetic resonance angiography (MRA)—an imaging test that does not use dyes or x rays and relies on special computer software and powerful magnetic fields to create a highly detailed image of the inside of the brain's arteries.
Preparation
If carotid ultrasonography or arteriography procedures were not performed earlier to diagnose carotid stenosis, these tests will be performed before surgery to evaluate the amount of plaque and the extent and location of narrowing in the patient's carotid arteries. Other blood vessels in the body are also evaluated. If other arteries show significant signs of artherosclerosis or damage, the patient's risk for surgery may be too great, and the procedure will not be performed. Aspirin therapy or other clot-prevention medication may be prescribed before surgery. Any underlying medical condition such as high blood pressure or heart disease will be treated prior to carotid endarterectomy to help achieve the best result from the surgery. Upon admission to the hospital , routine blood and urine tests will be performed.
Aftercare
A person who has had carotid endarterectomy will be monitored in a hospital recovery room immediately after the surgery and will then go to an intensive care unit at least overnight to be observed for any sign of complications. The total hospital stay may be two to three days. When the patient returns home, activities can be resumed gradually, as long as they are not strenuous. During recuperation, the patient's neck may ache slightly. The doctor may recommend against turning the head often or too quickly during recovery. The most important thing people can do after endarterectomy is to follow their doctor's guidelines for stroke prevention, which will reduce the progression of artherosclerosis and avoid repeat narrowing of the carotid artery. Repeat stenosis (restenosis) has been shown to occur frequently in people who do not make the necessary changes in lifestyle such as in diet, exercise , and quitting smoking or excessive use of alcohol. The benefits of the surgery may only be temporary if underlying disease such as artherosclerosis high blood pressure, or diabetes, is not also treated.
Risks
Serious risks are associated with carotid endarterectomy. They involve complications that can arise during or following the surgery, as well as underlying conditions that led to blockage of the patient's arteries in the first place. Stroke is the most serious postoperative risk. If it occurs within 12 to 24 hours after surgery, the cause is usually an embolism, which is a clot or tissue from the endarterectomy site. Other major complications that can occur are:
- heart attack or other heart problems
- death
- breathing difficulties
- high blood pressure
- nerve injury, which can cause problems with vocal cords, saliva management, and tongue movement
- bleeding within the brain
- restenosis, the continuing buildup of plaque, which can occur from five months to 13 years after surgery
The risks of carotid endarterectomy surgery depend upon age, overall health, and the skill and experience levels of the surgeons treating the patient. The likelihood of complications is lower when the surgeon performing the procedure has acknowledged skills and experience. According to the Stroke Council of the American Heart Association, surgery is best performed by a surgeon who has only had complications occur in less than 3% of patients. Hospitals, too, should be able to show that fewer than 3% of their patients undergoing endarterectomy have had complications. These recommendations are based not only on skill levels, but also on the ability to accurately weigh the stroke risks for each patient against the potential risk of complication because of age, hereditary factors, and the presence of underlying conditions or diseases.
Normal results
The desired outcome of carotid endarterectomy is improved blood flow to the brain and a reduced risk of stroke. The National Stroke Association has reported that successful carotid endarterectomy surgery reduces risk of stroke by as much as 80% in people who have had either transient ischemic attacks or symptoms of stroke, or who have been diagnosed with 70% or more arterial blockage. Studies of people who have no symptoms but have been found to have stenosis from 60% to 99%, show that endarterectomy surgery also reduces the risk of stroke by more than 50%. These groups of people at higher risk for stroke will benefit most from having carotid endarterectomy. The benefit for people who have lesser degrees of blockage is shown to be much lower than that of high-risk stroke candidates. Surgery is not indicated for people with artery narrowing less than 50%.
Morbidity and mortality rates
Death and disabling stroke occur more often in symptomatic and asymptomatic patients at high risk for stroke who have not been treated with carotid endarterectomy surgery. A well-respected study, the North American Symptomatic Carotid Endarterectomy Trial (NASCET), along with a corresponding European study (ECST), showed that death or disabling stroke are reduced by 48% among those with severe stenosis (greater than 70%) when they undergo carotid endarterectomy surgery. In patients with less severe stenosis (50–69%), endarterectomy was shown to reduce risk by 27%. Patients with less than 50% stenosis were actually harmed by surgery, increasing the risk of death or disability by 20%. The conclusion of the study was that death and disability could be reduced overall if carotid endarterectomy was performed only on patients with the more severe stenosis who are also surgically fit, and that that the procedure should be performed only by surgeons whose complication rates are less than 6%.
Alternatives
The carotid endarterectomy removes plaque directly from blocked arteries and there is no alternative way to mechanically remove plaque. However, there are alternative ways to prevent the buildup of plaque and thus help to prevent stroke or heart attack. Certain vitamin deficiencies in older people are known to promote high levels of homocysteine, an amino acid that contributes to atherosclerosis, putting people at greater risk for stroke or heart attack. Certain nutritional supplements have been shown to reduce homocysteine levels.
Nutritional supplements and alternative therapies that are sometimes recommended to help reduce risks and promote good vascular health include:
- Folic acid, which helps lower homocysteine levels and increases the oxygen-carrying capacity of red blood cells.
- Vitamins B 6 and B 12 , which help lower homocycteine levels; B6 is also a mild diuretic and helps to balance fluids in the body.
- Antioxidant vitamins C and E, which work together to promote healthy blood vessels and improve circulation.
- Angelica, an herb that contains coumadin, a recognized anticoagulant, which may help to prevent clot formation in the blood (blood thinner).
- Essential fatty acids, which help reduce blood pressure and cholesterol, and maintain elasticity of blood vessels.
- Chelation therapy, which can be used to break up plaque and improve circulation.
Resources
books
Caplan, L. R. American Heart Association Family Guide to Stroke Treatment, Recovery, and Prevention. New York: Times Books, 1994.
Moore, R. D. The High Blood Pressure Solution: A Scientifically Proven Program for Preventing Strokes and Heart Disease, 2nd Edition. Portland, OR: Inner Traditions, 2001.
periodicals
Harrar, S. "Brain Attack." Prevention Magazine 20 September 2002.
organizations
National Institute of Neurological Disorders and Stroke (NINDS). National Institutes of Health, Bethesda, MD 20892. http://www.ninds.nih.gov .
National Stroke Association. 9707 E. Easter Lane, Englewood, CO 80112. (800) Strokes or (303) 649-9299. http://www.stroke.org .
other
Carotid Endarterectomy: Questions and Answers. Harvard Medical School and Aetna. http://www.intelihealth.com .
Carotid Endarterectomy: What to Think About. Healthwise, Inc., Boise, ID. http://www.laurushealth.com/newsearch .
Uncontrollable Stroke Risk Factors and Controllable Stroke Risk Factors. National Stroke Association, Stroke Prevention Guidelines. http://www.stroke.org .
L. Lee Culvert
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Carotid endarterectomy is performed in a hospital or medical center operating room by a vascular surgeon or neurosurgeon.
QUESTIONS TO ASK THE DOCTOR
- Why do I need this surgery?
- How will the surgery improve my condition?
- What kind of anesthesia will I be given?
- What are the risks of having this surgery?
- Is there anything I can do, myself, to get in shape for the surgery and to improve my chances of successful surgery?
- How many of these procedures have you performed? How many of the surgery patients had complications after surgery?
- How can I expect to feel after surgery? How long will it take me to recover?
- What are my chances of developing this problem again after the surgery?
- If the surgery is not successful, what will my options be?
Thank you,
Best regards,
Y. Nomi
Sincerely,
V. Allen
Thank you.
I guess this is the best info I can get {and give} on the surgery.
Andrea
I am 78 yoa and in relatively good health. I think that the above history places me at a greater risk than usual. Do you have any suggestions? I'm ready to go do it.
Thank you.
Sam Litzenberg
would be less risky?
My question is exists any therapy to reduce the problem not necesarily surgery?
One day in this december 2010 he felt dizzy and his left hand dormed so we went to emergency
and after exams we knew about the corotids.
He has no colesterol and his blood presure in controled with medicine and he has no other problems. Please any specialized doctor who reads this , let me know what to do.
I´ll be waiting and thanks a lot.
Niky
You have to get well soon being as we are going to Mexico in the Spring. And YES, I have my passport stuff all ready to submit.
Love you guys
Mary Kaye and Nick
Carmen
Just had a carotid endarterectomy (CEA) surgical procedure done on my right side 5 days ago which had about an 80-90% blockage. Stayed in the ICU for two days until they could get my blood pressure stabilized. Heart rate and BP was running low after surgery. My cardioligist took me off all my high blood pressure medications and I'm being monitored to see when and if my BP gets back to around 150/ so he can start me on probably some new types of BP medications.
Staples should be removed in about 10 more days and hopefully I'll be back to work around that time.
NUMBNESS IN THE RIGHT SIDE OF HIS LIP. COULD YOU TELL ME WHAT IS TO BE EXPECTED ??
I HAD A ENDARTERECTOMY 6 WEEKS AGO MY JAW IS STILL NUMB AND NOW I HAVE GOT A VERY BAD PAIN IN MY SHOULDER BLADE AND COLLER BONE ,
IS THIS NORMAL
No history of stroke.
He is worried that since the operation 5 months ago his neck is constantly numb
from the right side of the neck all around the back to the left side neck
and up from under his right ear to the top of his head.
It is very numb on awakening after sleep and reduces somewhat as the day progresses but never goes away.
Your comments and advices will be much appreciated.
4 weeks later and still getting loads of pain and the numbness in my neck and face is so unreal, like I'm been hacked at all the time and having muscular spasms as well.
Love to hear from more people who have recently had same done
4 MONTHS SINCE LEFT ENDARTERECTOMRY.
STILL CANT SPEAK ABOVE WHISPER.
RIGHT DONE 15 YEARS AGO WITHOUT AMU PROBLEM.
since surgery. otherwise I feel fine
Thank you
Jeffrey Johnston
Thank you
I read post operation, nevk pain, speech problem, is it worth it to go through when this problem occurs. Stroke is worst if not done. Please advise. A
a direct question; does this situation calls for an immediate surgery, or it is recommended to treat with aspirin and to wait 6 months?
used a vein in my right leg above my ankle to cover the left side of my neck as my veins were very small. The operation was very succesful. I
was very tired after the survery after two nights in the hospital but the neck healed quickly but my leg where the vein was removed took three months before I could walk without pain. One surgeon did the neck another surgeon removed the vein all at the same time and fortunately
I did not need a shunt. Good luck to you if you need this surgery.