Dilatation and curettage
Definition
Dilatation and curettage (D & C) is a gynecological procedure in which the cervix is dilated (expanded) and the lining of the uterus (endometrium) is scraped away.
Purpose
D & C is used to diagnose and treat heavy or irregular bleeding from the uterus. Possible reasons for abnormal uterine bleeding include:
- Hormonal imbalance. Often women with abnormal bleeding are first treated with hormones in an attempt to normalize bleeding. D & C may be used to determine the cause of bleeding if hormone treatment is ineffective.
- Endometrial polyps. Polyps are benign growths that may protrude from the uterus by a stem or stalk, usually to the endometrium or cervix. D & C may be used to diagnose polyps or to remove them.
- Uterine fibroids. Also called leiomyomas, fibroids are benign growths in the smooth muscle of the uterus. Abnormal bleeding is often the only symptom of fibroids. D & C is often used to diagnose fibroids and may be used to scrape away small tumors; additional surgery may be needed to remove more extensive growths.
- Endometrial hyperplasia (EH). EH is a condition where the endometrium grows excessively, becoming too thick and causing abnormal bleeding. Tissue samples procured during D & C can be assessed for early signs of cancer.
- Cancer. D & C may be used to obtain tissue for microscopic evaluation to rule out cancer. Women over the age of 40 are at an increased risk of developing endometrial cancer.
- Miscarriage, incomplete abortion, or childbirth. Abnormal bleeding may result if some of the products of pregnancy remain in the uterus after a miscarriage or induced abortion, or if parts of the placenta are not expelled naturally after childbirth. These retained products can be scraped out by D & C.
Description
D & C is usually performed under general anesthesia, although local or epidural anesthesia can also be used.
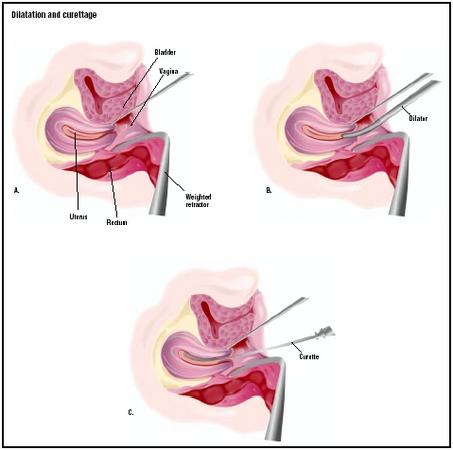
During the procedure (which takes only minutes to perform), the doctor inserts an instrument called a speculum to hold open the vaginal walls, and then stretches the opening of the uterus (the cervix) by inserting a series of tapering rods, each thicker than the previous one, or by using other specialized instruments. This process of opening the cervix is called dilation.
Once the cervix is dilated, the physician inserts a spoon-shaped surgical device called a curette into the uterus. The curette is used to scrape away the uterine lining. One or more small tissue samples from the lining of the uterus or the cervical canal are sent for analysis by microscope to check for abnormal cells.
Although simpler, less expensive techniques such as a vacuum aspiration are quickly replacing the D & C as a diagnostic method, it is still often used to diagnose and treat a number of conditions.
Diagnosis/Preparation
If general anesthesia will be used, the patient will be instructed to refrain from eating and drinking for at least eight hours before the procedure. The doctor may order blood and/or urine tests to scan for certain abnormalities. Because opening the cervix can be painful, sedatives may be given before the procedure begins. Deep breathing and other relaxation techniques may help ease cramping during cervical dilation.
Aftercare
A woman who has had a D & C performed in a hospital can usually go home the same day or the next day. Many women experience backache and mild cramps after the procedure, and may pass small blood clots for a day or so. Vaginal staining or bleeding may continue for several weeks.
Most women can resume normal activities almost immediately. Patients should avoid sexual intercourse, douching, and tampon use for at least two weeks to prevent infection while the cervix is closing and to allow the endometrium to heal completely.
Risks
The primary risk after the procedure is infection. If a woman experiences any of the following symptoms, she should report them immediately to her doctor, who can treat the infection with antibiotics:
- fever
- heavy bleeding
- severe cramps
- foul-smelling vaginal discharge
D & C is a surgical operation that has certain risks associated with general anesthesia such as pulmonary aspiration and failed intubation. Rare complications include perforation of the uterus (which usually heals on its own) or puncture of the bowel or bladder (which requires further surgery to repair).
Extensive scarring of the uterus may occur after over-aggressive scraping during D & C, leading to a condition called Asherman's syndrome. The major symptoms of Asherman's syndrome are light or absent menstrual periods, infertility, and recurrent miscarriages. Scar tissue can be removed with surgery in most women, although approximately 20–30% of women will remain infertile after treatment.
Normal results
Removal of the uterine lining will normally cause no side effects, and may be beneficial if the lining has thickened so much that it causes heavy periods. The uterine lining soon grows again normally, as part of the menstrual cycle.
Morbidity and mortality rates
D & C has been associated with a 4–10% rate of postoperative complications.
Alternatives
There are a number of alternatives to D & C, depending on the reason for doing the procedure. The following are some examples of procedures that allow doctors alternative ways of evaluating, sampling, or treating disorders of the inner lining of the uterus:
- Expectant management of spontaneous abortion. D & C is the most commonly used method of treatment for incomplete abortion; one study showed that over 90% of women who visited hospital emergency rooms for incomplete spontaneous abortion were treated by D & C. Recent studies, however, have shown that expectant management (i.e., no active intervention) is a viable option for women who do not wish to undergo surgery and who are in otherwise good health. Up to 72% of women indicated that that expectant management of incomplete abortion was preferable to medical or surgical intervention.
- Endometrial biopsy. This procedure is similar to D & C in that a curette is used to obtain a sample of endometrial tissue. Little or no cervical dilation is necessary, however, because the curette used in endometrial biopsy is narrower. The cervix is numbed with a local anesthetic but the patient will still experience cramping.
- Vacuum scraping. A thin plastic tube attached to a suction machine is passed through the cervix and scraped along the endometrium. Vacuum scraping has been shown to have similar success in diagnosing uterine cancer as D & C. Local anesthesia is also used for this procedure.
- Hysteroscopy. A thin telescope called a hysteroscope is inserted through the cervix and used to view the inside of the uterus after it has been expanded with a liquid or gas. The view afforded by the hysteroscope can help to diagnose abnormal growths, accumulation of scar tissue, or other conditions.
- Hysterectomy . A total hysterectomy permanently removes the uterus and cervix. This procedure is generally recommended only if a woman no longer desires to have children and no other forms of treatment have been successful. Most hysterectomies are done to treat uterine fibroids and endometriosis (a condition in which the endometrium grows outside of the uterus).
Resources
periodicals
Geyman, John, Lynn Oliver, and Sean Sullivan. "Expectant, Medical, or Surgical Treatment of Spontaneous Abortion in First Trimester of Pregnancy?" Journal of the American Board of Family Practice 12, no. 1 (1999): 55–64.
Molnar, Alexandra, Lynn Oliver, and John Geyman. "Patient Preferences for Management of First-Trimester Incomplete Spontaneous Abortion." Journal of the American Board of Family Practice 13, no. 5 (2000): 333–337.
organizations
American College of Obstetricians and Gynecologists. 409 12th St., SW, PO Box 96920, Washington, DC 20090-6920. http://www.acog.org
other
"Asherman's Syndrome." International Adhesions Society . April 24, 2002 [cited February 24, 2003]. http://www.adhesions.org/relatedconditions/asherman.htm .
"Dilatation and Curettage." eTenet . 2001 [cited February 24, 2003]. http://www.etenet.com/Apps/Library/Corporate.asp?ID=713 .
"Dilatation and Curettage." Patient Education Institute . December 21, 2001 [cited February 24, 2003]. http://www.nlm.nih.gov/medlineplus/tutorials/dilationandcurettage/og059101.html .
"Dysfunctional Uterine Bleeding." WomenOne.org . 2001 [cited February 24, 2003. http://www.womenone.org/health04.htm .
"Endometrial Hyperplasia." American College of Obstetricians and Gynecologists . 2001 [cited February 24, 2003]. <http://www.medem.com/MedLB/article_detaillb.cfm? article_ID=ZZZ7Z2GWQMC&sub_cat=9> .
"Hysterectomy." American College of Obstetricians and Gynecologists . 2001 [cited February 24, 2003]. http://www.medem.com/search/article_display.cfm?path=n:&mstr=/ZZZ MULQGSWC.html&soc=ACS&srch_typ=NAV_SERCH .
"Hysteroscopy." American College of Obstetricians and Gynecologists . 2001 [cited February 24, 2003]. <http://www.medem.com/MedLB/article_detaillb.cfm?article_ID=ZZZ AXX8MA7C&sub_cat=8> .
Williams, Carmine. "Dilation and Curettage." eMedicine . April 26, 2001 [cited February 24, 2003]. http://www.e medicine.com/aaem/topic156.htm .
Carol A. Turkington Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
D & C is generally performed by an obstetrician/gynecologist, a medical doctor who has completed specialized training in the areas of women's general health, pregnancy, labor and childbirth, prenatal testing, and genetics. Samples of the uterine lining may be sent to a pathologist for analysis. A pathologist is a medical doctor who has completed specialized training in the diagnosis of diseases from microscopic analysis of cells and tissues.
The health of the patient and the type of anesthesia used determines where a D & C is performed. The procedure is generally done in a hospital on an outpatient setting.
QUESTIONS TO ASK THE DOCTOR
- Why is D & C recommended for my condition?
- Where will the procedure be performed?
- What alternative therapies are available to me?
- What are my options in terms of anesthesia during the procedure?
- What risks are involved with the procedure?
Could you tell me the reference please? Thanks you very much
I went to my regular gynecologist today to make an appointment for him to do a D&C with a hysterscopy. I had been at his office September 14 or so the day I got my September 1 transvaginal ultrasound report. He told me about risks with the D&C such as bleeding,and that he could puncture my uterus or intestines etc. He said in his 20 years of doing D&C's it's never happened.He had asked me to sign consent forms but I got really scared then and he said OK you think about it.Well I had an appointment with him a few weeks ago but I had to cancel it because I got a very bad cold.
So he actually said when I came there to agree to go through with this procedure,when I said that I want an epidural and don't want to be put to sleep,he said it was fine but he said they may have to sedate you. I said why,he said if you start kicking and screaming,I said why would I kick and scream,he said you are a very anxious person,he said you don't consider yourself a very anxious person? He said I never had anyone have to come back four times to make a decision about getting something like this. I said it wasn't four times,the last time I came here was when I had just got back my recent transvaginal ultrasound and I was more concerned because this time it was four days after my period was over and my lining was too thick when it shouldn't have been.And I said my mother died as I told you of uterine cancer at age 49,and I have never had a procedure like this before.
At one point he said do you want someone else to do this? I said no,but I really wish I knew of another good and a nice doctor to do it! I had discussed this or getting a biopsy(he only uses the TruTest Tao brush biopsy which he gave me two years ago because endometrial cells had turned up on my pap test only two days after my period had ended but he said he would use the regular uterine biopsy if I wanted to and he would prescribe prescription pain medicine for it,but he said he could go in there with a brush or the other biopsy and miss the polyp)) done with him on the phone 2 times over months.
The gyneocologist said that he's not going to remove that much uterine lining,just a part of it and remove the polyp.
Also,In this recent report the radiologist said that the differential diagnoses is endometrial hyperplasia, a polyp or endometrial cancer my lining was 14mm just four days after my period ended.
Anyway, I was just hoping that you could offer any alternative suggestions if you have any.
Having had a D&C myself, I can say that general anesthesia is the way to go. And it's really not bad. They give you a light sedative by IV and then put a mask over your mouth and nose and ask you to breath deeply and then you're out. The next second (or so it feels!), you wake up in the recovery room, all fixed up. I've had two general anesthetics in my life and both experiences were like that. If I had to choose that route over experiencing any of the tugging and cramping sensations of a procedure, I'd choose the GA right away - it's much less scary! (The other nice think about GA is that you actually become alert quite quickly in recovery unlike when they just sedate you). Don't let yourself get too worked up about the procedure. It's low risk and very routine for gynecologists. All of this is a small price to pay for early treatment of a possible problem.
Wishing you courage, strength, and confidence to get this procedure done!
Regards,
Irene
its up to a month now that i had D&C is getting to 1 month and 1 week i still have seen my mestral cycle, what is wrong with me pls...should i still be excepting it or wat...pls i need ur advise. thanks. hoping to here from u.
and before using these dilater, how do the user know which size is determined, is there any other device to use before dilater(like fitting set).
Which positions are for cervical & virginal dilater.
Thanks in advance for your reply!
Pls i need ur advice,dis is my second time of having d & c operatn as an abortion.A day after d act, my breast grew bigger and harder,i went back 2 d hospital where i had it,d doctr tld me not to wory dat within a week it wil return 2 normal.Pls im worried.
Can i also do another d nd c this month or is there any trusted drugs that will put an end to it if it is pregnancy?
I have a very low tolerance for pain. Even at dentist..they always end up administrating more than that they thougt I would need. How to I go about finding a gyn or surgeon that is willing to accomadate me. My friend had procedure 6 mos ago. Doctor didn't inform her as to what he was doing. She said she screamed, then cried. Never felt pain like that before. She asked, why would doctors put women throught that without giving them something for pain. It was cruel.
My question is how to find a gyn or surgeon that will help me using some type of sedation for the biospy?
Don't feel comfortable going back to this hospital, feeling a bit traumatized, also wish I had asked for more details from Dr. Still having cramps.