Disk removal
Definition
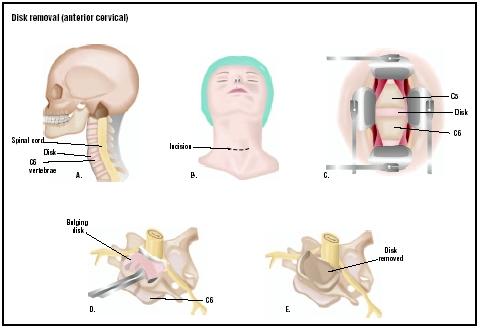
Disk removal is one of the most common types of back surgery. Diskectomy (also called discectomy) is the removal of an intervertebral disk, the flexible plate that connects any two adjacent vertebrae in the spine. Intervertebral disks act as shock absorbers, protecting the brain and spinal cord from the impact produced by the body's movements.
Purpose
Removing the invertebral disk is performed after completion of unsuccessful conservative treatment for back pain that has been present for at least six weeks. Surgery is also performed if there is pressure on the lumbosacral nerve roots that causes weakness, bowel dysfunction, or bladder dysfunction.
As a person ages, the disks between vertebrae degenerate and dry out, and tears form in the fibers holding them in place. Eventually, the disk can develop a blister-like bulge, compressing nerves in the spine and causing pain. This is called a "prolapsed" (or herniated) disk. If such a disk presses on a nerve root and causes muscle weakness, or problems with the bladder or bowel, immediate disk removal surgery may be needed.
The goal of the surgery is to relieve all pressure on nerve roots by removing the pulpy material from the disk, or the entire disk. If it is necessary to remove material from several nearby vertebrae, the spine may become unsteady. In this case, the surgeon will perform a spinal fusion , removing all disks between two or more vertebrae, and roughening the bones so that the vertebrae heal together. Bone strips taken from the patient's leg or hip may be used to help hold the vertebrae together. Spinal fusion decreases pain, but decreases spinal mobility.
Demographics
Approximately 150,000 Americans undergo disk removal each year in the United States.
Description
The surgery is performed under general anesthesia. The surgeon cuts an opening into the vertebral canal, and moves the dura and the bundle of nerves called the "cauda equina" (horse's tail) aside, which exposes the disk. If a portion of the disk has moved out from between the vertebrae and into the nerve canal, it is simply
There are minimally invasive surgical techniques for disk removal, including microdiskectomy. In this procedure, the surgeon uses a magnifying instrument or special microscope to view the disk. Magnification makes it possible to remove a herniated disk with a smaller incision, causing less damage to nearby tissue. Video-assisted arthroscopic microdiskectomy has exhibited good results with less use of narcotics and a shortened period of disability. Newer forms of diskectomy are still in the research stage, and are not yet widely available. These include laser diskectomy and automated percutaneous diskectomy.
Total disk replacement research in the United States is underway. Products under investigation include the ProDisc (made by Spine Solutions, Inc.), and the SB Charite III (made by Link Spine Group, Inc.). In these clinical studies, a significant number of patients who received artificial disk implants report a reduction in back and leg pain; 92.7% state they are satisfied or extremely satisfied with the procedure.
Diagnosis/Preparation
The physician will obtain x rays and neuroimaging studies, including a computed tomography (CT) scan, myelogram, and magnetic resonance imaging (MRI); and clinical exams to determine the precise location of the affected disk.
An hour before surgery, the patient is given an injection to dry up internal fluids and encourage drowsiness.
Aftercare
After the operation, the patient is lying flat and face down when he or she awakens. This position must be maintained for several days, except for occasional positional changes to avoid bedsores . There may be slight pain or stiffness in the back area.
Patients usually leave the hospital on the fourth or fifth day after surgery. They must:
- Avoid sitting for more than 15–20 minutes.
- Use a reclined chair.
- Avoid bending at the waist, twisting, or lifting heavy objects.
- Begin gentle walking (indoors or outdoors), and gradually increase exercise . Exercise should be continued for the next four weeks.
- Begin stationary biking or gentle swimming after two weeks.
- Sleep on a firm mattress.
- Slow down if they experience more than minor pain in the back or leg.
- Refrain from sitting in one place for an extended period of time (e.g., long car ride).
Patients should be able to resume normal activities in four to six weeks.
Risks
All surgery carries some risk due to heart and lung problems or the anesthesia itself, but this risk is generally very small. (The risk of death from general anesthesia for all types of surgery, for example, is only approximately one in 1,600 surgeries.)
The most common risk of the surgery is infection, which occurs in 1–2% of cases. Rarely, the surgery damages nerves in the lower back or major blood vessels in front of the disk. Occasionally, there may be some residual paralysis of a leg or bladder muscle after surgery, but this is the result of the disk problem that necessitated the surgery, not the operation itself.
Normal results
In properly evaluated patients, there is a very good chance that disk removal will be successful in easing pain. The surgery can relieve pain in 90% of cases; however, there are some people who do not achieve pain relief. This depends on a number of factors, including the length of time that they had the condition requiring surgery. Disk surgery has a "good to excellent" result in 87% of patients over age 60. The surgery can relieve both back and leg pain, especially the latter.
Alternatives
Prior to disk removal surgery, a patient usually undergoes treatment with medical or physical therapy. Disk removal surgery may be indicated if these treatments are ineffective, or if emergency symptoms (i.e., bladder and bowel dysfunction) develop.
See also Bone grafting ; Spinal fusion .
Resources
books
Beauchamp, M.D., Daniel R., Mark B. Evers, M.D., Kenneth L. Mattox, M.D., Courtney M. Townsend, and David C. Sabiston (Editors). Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 16th edition. London: W B Saunders Co., 2001.
Bogduk, Nikolai, Brian McGuirk, and Boriana Dirk Van Der Deliiska. Medical Management of Acute and Chronic Low Back Pain. Philadelphia, PA: Elsevier Health Sciences, 2002.
Cailliet, Rene. Low Back Disorders: A Medial Enigma. Philadelphia, PA: Lippincott Williams & Wilkins, 2003.
Lawrence, Peter F., Richard M. Bell, and Merril T. Dayton, eds. Essentials of General Surgery. 3rd edition. Philadelphia, PA: Lippincott, Williams & Wilkins, 2000.
Resnick, Daniel K., ed. Surgical Management of Low Back Pain (Neurosurgical Topics). 2nd edition. Rolling Meadows, IL: American Association of Neurological Surgeons, 2001.
Watkins, Robert G. Surgical Approaches to the Spine. 2nd edition. Berlin, Germany: Springer Verlag. 2003.
periodicals
Alini, M., P. J. Roughley, J. Antoniou, T. Stoll, and M. Aebi. "A Biological Approach to Treating Disc Degeneration: Not for Today, But Maybe for Tomorrow." European Spine Journal 11, no. 2 (October 2002): S215-20.
Deyo, R., and J. Weinstein. "Low Back Pain." New England Journal of Medicine 344, no. 5 (2001): 363-70.
Oskouian, R .J., Jr., J. P. Johnson, and J. J. Regan. "Thoracoscopic Microdiscectomy." Neurosurgery 5, no.1 (January 2002): 103-9.
Silber, J. S., D. G. Anderson, V. M. Hayes, and A. R. Vaccaro. "Advances in Surgical Management of Lumbar Degenerative Disease." Orthopedics 25, no.7 (July 2002): 767-71.
organizations
North American Spine Society. 22 Calendar Court, 2nd Floor, LaGrange, IL 60525. (877) Spine-Dr. E-mail: info@ spine.org. http://www.spine.org .
National Institutes of Health. 9000 Rockville Pike, Bethesda, MD 20892. (301) 496-4000. Email: NIHInfo@od.nih. gov. http://www.nih.gov/ .
other
Spine Health.com . Total Disc Replacement. 2003. http://www.spine-health.com/research/discupdate/artificial/artificial04.html . [cited March 19, 2003].
American Academy of Orthopaedic Surgery (AAOS) and American Association of Orthopaedic Surgery. Low Back Surgery. 2001. http://orthoinfo.aaos.org/booklet/thr_report.cfm?thread_id=10&topcategory=sp . [cited March 19, 2003].
Carol A. Turkington Crystal H. Kaczkowski, MSc.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Disk removal is performed by an orthopedic surgeon or neurosurgeon in a hospital setting.
QUESTIONS TO ASK THE DOCTOR
- Is disk removal the only option available?
- What results are anticipated?
- How many disk removal surgeries has the surgeon performed?
- What are the risks?
SLIGHTLY WORRIED HAVING HAD MRI BEIN TOLD I HAVE 5 BAD DISKS 1 COMPLETLY PROLAPSED GREAT ! JUST READ YOUR INFO IT HAS ANSWERED MOST QUESTIONS THANKS . PAT BRIGGS
Questiona:
a) How often the infection occurs
b) Is the residual pain primarily due to the infection
c) How much time it will take before the infection goes away. (Its already 90 days now)
-PKG
any problems accuring when,i return to work as i do a heavy
lifting manual job.any guidlines,which could help
thank you
After all the pain for the last 5months, I am looking forward to the surgery and putting my faith in God for a great outcome. Wish me luck!