Femoral hernia repair
Definition
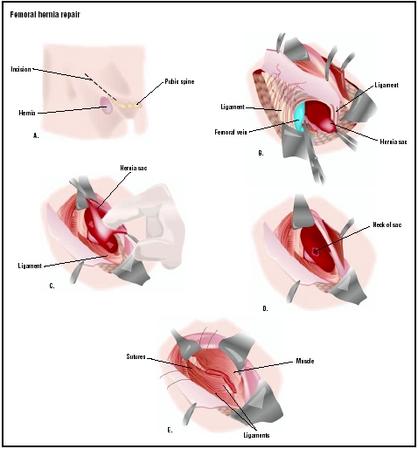
A femoral hernia repair, or herniorraphy is a surgical procedure performed to reposition tissue that has come out through a weak point in the abdominal wall near the groin. In general, a hernia is a protrusion of a loop or piece of tissue through a weak spot or opening in the abdominal wall. There are several different kinds of hernias; they are named according to their location. A femoral hernia is one that occurs in a person's groin near the thigh. In a child, a femoral hernia is usually the result of incomplete closing of this area during development in the womb.
Purpose
Femoral hernia repair is done to reduce the patient's risk of a future surgical emergency. A hernia may be congenital (present at birth) or may develop later in life because of a weakness in the abdominal wall. If the opening is very small, the amount of tissue that can push through it is small, and the person may barely be aware of the problem. One complication that may arise, however, is that the tissue that comes out through the opening can become incarcerated, or trapped. If the herniated tissue has its blood supply diminished because of pressure from other nearby organs or structures, it is referred to as strangulated. Strangulation may lead to gangrene, which means that the affected tissue can die and be invaded by bacteria. Femoral hernias are more likely than other hernias to become incarcerated or strangulated because the affected tissue pushes through a relatively small and closely confined space. Because of the increased risk of eventual strangulation and gangrene, the patient's doctor may recommend surgical repair of the hernia.
Demographics
Femoral hernias are a relatively uncommon type, accounting for only 3% of all hernias. While femoral hernias can occur in both males and females, almost all of them develop in women because of the wider bone structure of the female pelvis. Femoral hernias usually grow larger over time; any activity that involves straining, such as heavy lifting or a chronic cough, may cause the hernia to enlarge. Poor abdominal muscle tone, obesity, and pregnancy also increase a woman's risk of developing a femoral hernia. Most femoral hernias develop on only one side of the patient's abdomen, but about 15% of femoral hernias are bilateral. These bilateral hernias are more likely to become strangulated. An additional 20% of femoral hernias become incarcerated.
Femoral hernias are more common in adults than in children. Those that do occur in children are more likely to be associated with a connective tissue disorder or with conditions that increase intra-abdominal pressure. Seventy percent of pediatric cases of femoral hernias occur in infants under the age of one.
Description
Femoral hernia repair may be performed under either general or local anesthesia. The repair of the hernia involves a cut, or incision, in the groin area (near the thigh), adjacent to the femoral artery. The surgeon locates the hernia, and reduces it by pushing the protruding tissue back inside the abdominal cavity. A hernia is referred to as reducible when the tissue that has come out through the opening can be pushed back and the opening closed. If incarceration or strangulation has occurred, the hernia is referred to as irreducible.
The procedure may be performed using the traditional open method, which requires a larger surgical incision, or by a laparoscopic approach. A laparoscopic procedure is performed through a few very small incisions. The hole in the abdominal wall may be closed with sutures, or by the use of a fine sterile surgical mesh. The mesh, which provides additional strength, is sewn into the abdominal wall with very small stitches. Some surgeons may choose to use the mesh when repairing a larger hernia. A hernia repair done with a mesh insert is called a tension-free procedure because the surgeon does not have to put tension on the layer of muscle tissue in order to bring the edges of the hole together. A laparoscopic hernia repair takes about 40 minutes to complete.
Diagnosis/Preparation
Diagnosis
A femoral hernia is usually diagnosed during a physical examination . In many cases, the patient will
In adult patients, the doctor will rule out the possibility that the pain is caused by an enlarged lymph node, a lipoma, or an inguinal hernia. Imaging studies are not generally used in diagnosing a hernia unless the doctor suspects that the hernia is incarcerated or strangulated. A strangulated hernia can be distinguished from an incarcerated hernia by the presence of fever; pain that persists after the doctor has reduced the hernia manually; and pain that is more severe than warranted by the examination findings.
Preparation
If the doctor suspects that the hernia is strangulated, he or she will give the patient a broad-spectrum antibiotic (usually cefoxitin) intravenously before the patient is taken to the operating room .
Adults scheduled for a nonemergency herniorraphy are given standard blood tests and a urinalysis . They should not eat breakfast on the morning of the procedure, and they should wear loose-fitting, comfortable clothing that they can easily pull on after the surgery without straining their abdomen.
Aftercare
Aftercare depends on several factors: the patient's age and general health status; the type of surgery (open or laparoscopic); and the type of anesthesia administered. Immediately after the procedure, the patient will be taken to the recovery area of the surgical center and monitored for signs of excessive bleeding, infection, uncontrolled pain, or shock. An uncomplicated femoral hernia repair is usually performed on an outpatient basis, which allows the patient to go home within a few hours of the surgery.
The patient will be given instructions about incision care , which will depend on the type of surgery and the way in which the incision was closed. Sometimes a transparent dressing is placed on the wound that the patient can remove about three days after the procedure. Very small incisions, such as those used for laparoscopic surgery, may be closed with Steri-strips® instead of sutures. The incision should be kept dry, so patients should take a sponge bath rather than a shower or tub bath for several days after surgery.
Adults should avoid heavy lifting for several weeks after a hernia repair. The surgeon can give the patient advice about specific weight limits on lifting. Contact sports and vigorous exercise should be avoided for about three weeks after a femoral hernia repair. Many patients will be able to return to most of their daily activities in a few days, with complete recovery taking about a month in patients without other medical conditions.
Risks
All surgical procedures have associated risks, both surgical and anesthesia-related. Bleeding and infection are the two primary surgical risks. The risk of infection for an uncomplicated femoral hernia repair is about 1%. Anesthesia-related risks include reactions to the anesthetic agents, including interactions with over-the-counter and herbal preparations, as well as potential respiratory problems. There is a small risk of recurrence of a femoral hernia. In addition, female patients are at some risk of injury to the nerves and blood supply of their reproductive organs, because femoral hernias develop in a part of the abdominal wall that is close to the uterus and ovaries.
Normal results
Normal results with timely diagnosis and repair of a femoral hernia are a smooth recovery with no recurrence of the hernia.
Morbidity and mortality rates
The mortality rate following an uncomplicated femoral hernia repair is essentially zero. The mortality rate for repair of a strangulated hernia that has necessitated a bowel resection is higher, however, ranging from 5–19%. Morbidity following an uncomplicated herniorraphy is low; one Danish study reported that the most common complication, reported by 8% of patients, was pain during procedures performed under local anesthesia. A British study of laparoscopic hernia repairs found that only 22 out of 3017 patients reported recurrence of the hernia. The incidence of postoperative swelling and bruising was 8%.
Alternatives
There are no medical or surgical alternatives to a femoral hernia repair other than watchful waiting. There is some risk that the hernia will enlarge, however, which increases the risk of incarceration or strangulation. Moreover, the complications and risks of surgery increase with incarcerated or strangulated hernias. Once a hernia is suspected or diagnosed, it should be evaluated by a surgeon within a month to lower the risk of complications.
See also Incisional hernia repair ; Inguinal hernia repair .
Resources
books
Ashcraft, Keith W. Pediatric Surgery . Philadelphia, PA: W. B. Saunders Company, 2000.
Delvin, David. Coping with a Hernia . London, UK: Sheldon Press, 1998.
periodicals
Callesen, T., K. Bech, and H. Kehlet. "Feasibility of Local Infiltration Anaesthesia for Recurrent Groin Hernia Repair." European Journal of Surgery 167 (November 2001): 851-854.
Kapiris, S. A., W. A. Brough, C. M. Royston, et al. "Laparoscopic Transabdominal Preperitoneal (TAPP) Hernia Repair. A 7-Year Two-Center Experience in 3017 Patients." Surgical Endoscopy 15 (September 2001): 972-975.
Kulah, B., A. P. Duzgun, M. Moran, et al. "Emergency Hernia Repairs in Elderly Patients." American Journal of Surgery 182 (November 2001): 455-459.
Manthey, David, MD. "Hernias." eMedicine , June 22, 2001 [June 6, 2003]. http://www.emedicine.com/EMERG/topic251.htm .
organizations
American Academy of Family Physicians. 11400 Tomahawk Creek Parkway, Leawood, KS 66211-2672. (913) 906-6000. E-mail: fp@aafp.org. http://www.aafp.org .
American Academy of Pediatrics. 141 Northwest Point Boulevard, Elk Grove Village, IL 60007-1098. (847) 434-4000. Fax: (847) 434-8000. E-mail: kidsdoc@aap.org. http://www.aap.org .
American College of Surgeons. 633 North St. Clair Street, Chicago, IL 60611-3231. (312) 202-5000. Fax: (312) 202-5001. http://www.facs.org .
other
Hernia Resource Center. http://www.herniainfo.com .
National Library of Medicine. http://www.nlm.nih.gov .
Esther Csapo Rastegari, R.N., B.S.N., Ed.M.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
This procedure is performed by a general surgeon. As with any procedure, the more experience the surgeon has with the particular surgery being performed, the better the expected outcome. A femoral hernia repair is usually performed on an outpatient, or ambulatory, basis in a hospital. After a few hours of recovery in the surgical center, the patient is able to return home.
QUESTIONS TO ASK THE DOCTOR
- How many femoral hernia repairs have you performed?
- Am I a candidate for laparoscopic surgery?
- How many femoral hernia repairs have you performed with a laparoscope?
- What kinds of complications have your patients experienced?
- How long is my recovery likely to take?
- What limitations will there be on my daily activities, such as returning to work, driving, or lifting a toddler?
I am currently 28 weeks pregnant and been diagnosed with a hernia and I can't find any information on this topic. I want to know will I have to have a c-section due to the hernia because a vaginal birth may make the hernia larger? If you have any information on this could you please email it to me at startingoveragain@hotmail.com
Greatly appreciated
I am due in 7 weeks and have a femoral hernia. Should I do a natural birth or is csection best? I don't want the hernia to get worse. Also I am o.k with a c-section, but my doctor will not tell me which will be the better option for me. Could you help me regarding this matter?
Kind Regards,
Mandy
I had bilateral (both sides) femoral hernias during my pregnancy. I ended up having a c-section as my obstetrician agreed there were more than just a few risks with going natural. He didn't want to sway me either way as they can't do that. I was fine with a c-section as it meant my bub would be safe - I wasn't willing to risk him. 1yr on hernia doesn't bother me much but am looking at getting pregnant again so am seeing a surgeon to see if they need fixing first. Towards the end of my pregnancy I was very uncomfortable with 2 of them and don't want that again with a toddler to run after! Good luck.
I have just had a femoral hernia repair two weeks ago it was nothing like the above info.. i had a large incision in the pubic region was in hospital for 5 days. i still have a dressing on it and i return to work in 4 weeks time thats 6 and a half weeks off work since i was rushed in as a emergency..it was diagnosed by my gp 4 weeks prior to my op.. was meant to have it done in day surgery but unfortunately became strangulated and became an emergency.. not a nice op and still struggling swelling is horendous ans still is never thought it would be like this.. but glads it over and done
Thank you
Marc Sorter
Surgeon
British Hernia Centre
Within three weeks after surgery I had this very huge bulge in the same location of incision on my left side. The VA doctor said that it was a femoral hernia. So they put a plug (Bard mesh perfix plug), it's rare in men I have read. I have returned back to work but so has a severe pain in the same area as the plug. Should I go and talk to my Dr? Or is my body adjusting to this plug in my body. It has been 6 -7 months since surgery.
Within three weeks after surgery I had this very huge bulge in the same location of incision on my left side. The VA doctor said that it was a femoral hernia. So they put a plug (Bard mesh perfix plug), it's rare in men I have read. I have returned back to work but so has a severe pain in the same area as the plug. Should I go and talk to my Dr? Or is my body adjusting to this plug in my body. It has been 6 -7 months since surgery.
My bowels haven't moved by themselves ever since I get constant bloating in my abdomen and it still feels rore inside along my groin area and across my pubic bone area
I've had a c t scan and also a colonoscopy but they haven't found anything which I'm puzzled about
I'm very concerned that something doesn't feel right inside and am worried that this is not being taken seriously
What is the solution now ?