Gastrostomy
Definition
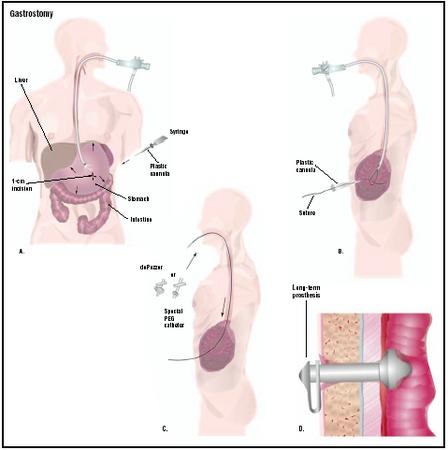
Gastrostomy is a surgical procedure for inserting a tube through the abdomen wall and into the stomach. The tube, called a "g-tube," is used for feeding or drainage.
Purpose
Gastrostomy is performed because a patient temporarily or permanently needs to be fed directly through a tube in the stomach. Reasons for feeding by gastrostomy include birth defects of the mouth, esophagus, or stomach, and neuromuscular conditions that cause people to eat very slowly due to the shape of their mouths or a weakness affecting their chewing and swallowing muscles.
Gastrostomy is also performed to provide drainage for the stomach when it is necessary to bypass a longstanding obstruction of the stomach outlet into the small intestine. Obstructions may be caused by peptic ulcer scarring or a tumor.
Demographics
In the United States, gastrostomies are more frequently performed on older persons. The procedure occurs most often in African-American populations.
Description
Gastrostomy, also called gastrostomy tube (g-tube) insertion, is surgery performed to give an external opening into the stomach. Surgery is performed either when the patient is under general anesthesia—the patient feels as if he or she is in a deep sleep and has no awareness of what is happening—or under local anesthesia. With local anesthesia, the patient is awake, but the part of the body cut during the operation is numbed.
Fitting the g-tube usually requires a short surgical operation that lasts about 30 minutes. During the surgery, a hole (stoma) about the diameter of a small pencil is cut in the skin and into the stomach; the stomach is then carefully attached to the abdominal wall. The g-tube is then fitted into the stoma. It is a special tube held in place by a disc or a water-filled balloon that has a valve inside allowing food to enter, but nothing to come out. The hole can be made using two different methods. The first uses a tube called an endoscope that has a light at the end, which is inserted into the mouth and fed down
The length of time the patient needs to remain in the hospital depends on the age of the patient and the patient's general health. In some cases, the hospital stay can be as short as one day, but often is longer. Normally, the stomach and abdomen heal in five to seven days.
The cost of the surgery varies, depending on the age and health of the patient. Younger patients are usually sicker and require more intensive, and thus more expensive, care.
Preparation
Prior to the operation, the doctor will perform an endoscopy and take x rays of the gastrointestinal tract. Blood and urine tests will also be performed, and the patient may meet with the anesthesiologist to evaluate any special conditions that might affect the administration of anesthesia.
Aftercare
Immediately after the operation, the patient is fed intravenously for at least 24 hours. Once bowel sounds are heard, indicating that the gastrointestinal system is working, the patient can begin clear liquid feedings through the tube. The size of the feedings is gradually increased.
Patient education concerning use and care of the gastrostomy tube is very important. Patients and their families are taught how to recognize and prevent infection around the tube; how to insert food through the tube; how to handle tube blockage; what to do if the tube pulls out; and what normal activities can be resumed.
Risks
There are few risks associated with this surgery. The main complications are infection, bleeding, dislodgment of the tube, stomach bloating, nausea, and diarrhea.
Gastrostomy is a relatively simple procedure. As with any surgery, however, patients are more likely to experience complications if they are smokers, obese, use alcohol heavily, or use illicit drugs. In addition, some prescription medications may increase risks associated with anesthesia.
Normal results
The patient is able to eat through the gastrostomy tube, or the stomach can be drained through the tube.
Morbidity and mortality rates
A study performed in 1998 on hospitalized Medicare beneficiaries aged 65 years or older who underwent gastrostomy revealed substantial mortality rates. The in-hospital mortality rate was 15.3%. Cerebrovascular disease, neoplasms, fluid and electrolyte disorders, and aspiration pneumonia were the most common primary diagnoses. The overall mortality rate at 30 days was 23.9%, reaching 63% at one year and 81.3% at three years.
Alternatives
There are no alternatives to a gastrostomy because the decision to perform it is made when a person is unable to take in enough calories to meet the demands of his or her body.
Resources
books
Griffith, H. Winter. Complete Guide to Symptoms, Illness, & Surgery, 3rd edition. New York: The Body Press/Perigee, 1995.
Ponsky, J. L. Techniques of Percutaneous Gastrostomy. New York: Igaku-Shoin Medical Pub., 1988.
periodicals
Angus, F., and R. Burakoff. "The Percutaneous Endoscopic Gastrostomy Tube. Medical and Ethical Issues in Placement." American Journal of Gastroenterology 98 (February 2003): 272–277.
Ciotti, G., R. Holzer, M. Pozzi, and M. Dalzell. "Nutritional Support Via Percutaneous Endoscopic Gastrostomy in Children with Cardiac Disease Experiencing Difficulties with Feeding." Cardiology of the Young 12 (December 2002): 537–541.
Craig, G. M., G. Scambler, and L. Spitz. "Why Parents of Children with Neurodevelopmental Disabilities Requiring Gastrostomy Feeding Need More Support." Developments in Medical Child Neurology 45 (March 2003): 183–188.
Niv, Y., and G. Abuksis. "Indications for Percutaneous Endoscopic Gastrostomy Insertion: Ethical Aspects." Digestive Diseases 20 (2002): 253–256.
organizations
American Gastroenterological Association (AGA). 4930 Del Ray Avenue, Bethesda, MD 20814. (301) 654-2055. http://www.gastro.org .
United Ostomy Association, Inc. (UOA). 19772 MacArthur Blvd., Suite 200, Irvine, CA 92612-2405. (800) 826-0826. http://www.uoa.org .
Tish Davidson, AM
Monique Laberge, PhD
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
The procedure is performed at a hospital or surgical clinic by a surgeon or gastroenterologist trained in endoscopy and placement of these tubes.
QUESTIONS TO ASK THE DOCTOR
- What happens on the day of surgery?
- What type of anesthesia will be used?
- What happens after g-tube insertion?
- What are the risks associated with the procedure?
- How is the g-tube insertion done?
- Will there be a scar?
- Will I be able to eat normal food?
- Will people notice that I have a g-tube?
- Will it be there forever?