Hypospadias repair
Definition
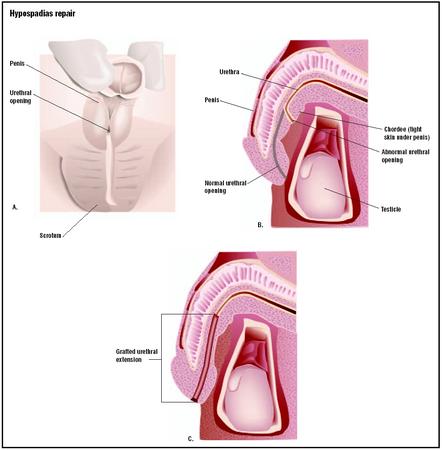
Hypospadias repair refers to a group of surgical approaches used to correct or reconstruct parts of the external genitalia and urinary tract related to a displaced meatus, or opening of the urethra. The urethra is the passageway that carries urine from the bladder to the outside of the body. Hypospadias is the medical term for a birth defect in which the urethra opens on the underside of the penis (in boys) or into the vagina (in girls). The word hypospadias comes from two Greek words that mean underneath and rip or tear, because severe forms of hypospadias in boys look like large tears in the skin of the penis.
Hypospadias is one of the most common congenital abnormalities in males. It was described in the first and second centuries A . D . by Celsus, a Roman historian of medicine, and Galen, a Greek physician. The first attempt to correct hypospadias by surgery was made in 1874 by Duplay, a French surgeon; as of 2003, more than 200 different procedures for the condition have been reported in the medical literature.
Hypospadias repair is, however, controversial because it is genital surgery. Some people regard it as unnecessary interference with a child's body and a traumatic experience with psychological consequences extending into adult life. Others maintain that boys with untreated hypospadias are far more likely than those who have had surgery to develop fears about intimate relationships and sexuality. There is little information about the emotional aftereffects of hypospadias repair on girls.
Purpose
Although there are several different surgical procedures used at present to correct hypospadias depending on its severity, all have the following purposes:
- To permit emptying of the bladder standing up. The abnormal location of the urethral meatus on the underside of the penis forces many boys to void urine sitting down, which leads to anxiety about using public restrooms or otherwise being seen undressed by other males.
- To correct a condition associated with hypospadias known as chordee. Chordee, which comes from the French cordée , which means tied or corded, is a condition in which the penis bends downward during an erection. This curving or bending makes it difficult to have normal sexual intercourse as an adult.
- To prevent urinary tract infections (UTIs). It is common in hypospadias for the urethral meatus to be stenotic, or abnormally narrowed. A stenotic urethra increases the risk of frequent UTIs.
- To lower the risk of developing testicular cancer. Hypospadias has been identified as a risk factor for developing testicular cancer after adolescence.
- To confirm the boy's sexual identity by improving the outward appearance of the penis. The external genitals of babies with severe hypospadias may look ambiguous at birth, causing stress for the parents about their child's gender identity.
Demographics
Hypospadias is much more common in males than in females. In Canada and the United States, the incidence of hypospadias in boys is estimated to be 1:250 or 1:300 live births. In girls, the condition is very rare, estimated at 1:500,000 live births. One troubling phenomenon is the reported doubling of cases of hypospadias in both Europe and North America since the 1970s without any obvious explanation. According to a recent press release from the U.S. Centers for Disease Control and Prevention (CDC), data from two surveillance systems monitoring birth defects in the United States show that the rate of hypospadias rose from 36 per 10,000 male births in 1968 to 80 per 10,000 male births in 1993. In addition to the increase in the number of cases reported, the proportion of severe cases has also risen, which means that the numerical increase cannot be explained as the result of better reporting.
The severity of hypospadias is defined according to the distance of the urethral opening from its normal location at the tip of the penis. In mild hypospadias, which is sometimes called coronal/glandular hypospadias, the urethral opening is located on the shaft of the penis just below the glans. In mild to moderate hypospadias, the opening is located further down the shaft of the penis toward the scrotum. In severe hypospadias, which is also called penoscrotal hypospadias, the urethral opening is located on the scrotum. About 80–85% of hypospadias are classified as mild; 10–15% as mild to moderate; and 3–6% as severe.
Although the causes of hypospadias are not yet fully understood, the condition is thought to be the end result of a combination of factors. The following have been associated with an increased risk of hypospadias:
- Genetic inheritance. Hypospadias is known to run in families; a boy with hypospadias has a 28% chance of having a male relative with the condition.
- Genetic disorders. Hypospadias is found in boys with a deletion on human chromosome 4p, also known as Wolf-Hirschhorn syndrome; and in persons with a variety of intersex conditions related to chromosomal abnormalities. Several different genetic mutations responsible for a deficiency in 5-alpha reductase, an enzyme needed to convert testosterone to a stronger androgen needed for urethral development, have been found in boys with hypospadias.
- Low birth weight. Several studies in the United Kingdom as well as in the United States have shown that male infants with hypospadias weigh less and are smaller at birth than controls. It is thought that these low measurements are markers of fetal androgen dysfunction.
- Drugs taken by the mother during pregnancy. Diethylstilbestrol (DES), a synthetic hormone that was prescribed for many women between 1938 and 1971 to prevent miscarriage, has been associated with an increased risk of stenosis of the urethral meatus as well as hypospadias in the sons of women who took the medication. Boys born to mothers addicted to cocaine also have an abnormally high rate of hypospadias.
- Environmental contamination. One proposal for explaining the rising rate of hypospadias and other birth defects in males is the so-called endocrine disruptor hypothesis. Many pesticides, fungicides, and other environmental pollutants contain estrogenic or anti-androgenic substances that interfere with the normal androgen pathways in embryonic tissue development—in birds and other animals as well as in humans.
- Assisted reproduction. A study done in Baltimore of children who were conceived through in vitro fertilization (IVF) between 1988 and 1992 found that the incidence of hypospadias among the males was five times that of male infants in a control group.
With regard to ethnic and racial differences in the American population, the CDC reports that Caucasians have the highest rates of hypospadias, Hispanics have the lowest, and African Americans have intermediate rates. Other studies have found that hypospadias is more common in males of Jewish or Italian descent than in other ethnic groups.
Description
Correction of hypospadias in boys
The specific surgical procedure used depends on the severity of the hypospadias. The objectives of surgery always include widening the urethral meatus; correcting chordee, if present; reconstructing the missing part of the urethra; and making the external genitalia look as normal as possible. Most repair procedures take between one-anda-half and three hours, and are performed under general anesthesia. Mild hypospadias can be corrected in a one-step procedure known as a meatal advancement and glanduloplasty, or MAGPI. In a MAGPI procedure, the opening of the urethra is moved forward and the head of the penis is reshaped. More severe hypospadias can also be corrected in one operation, which involves degloving the penis (separating the skin from the shaft) in order to cut the bands of tissue that cause chordee, and constructing a new urethra that will reach to the tip of the penis. The specific technique of reconstruction is usually decided in the operating room , when the surgeon can determine how much tissue will be needed to make the new urethra. In some cases, tissue must be taken from the inner arm or the lining of the mouth. In a few cases, the repair may require two or three stages spaced several months apart.
There is some remaining disagreement among professionals regarding the best age for hypospadias repair in boys. Most surgeons think the surgery should be done between 12 and 18 months of age, on the ground that gender identity is not fully established prior to toilet training and the child is less likely to remember the operation. Some doctors, however, prefer to wait until the child is about three years old, particularly if the repair involves extensive reconstruction of the urethra.
Recent advances in hypospadias repair include the use of tissue glues and other new surgical adhesives that speed healing and reduce the risk of fistula formation. In addition, various synthetic materials are being tested for their suitability in constructing artificial urethras, which would reduce the risk of complications related to skin grafting .
Correction of hypospadias in girls
The most common surgical technique for correcting hypospadias in girls is construction of a new urethra that opens to the outside of the body rather than emptying into the vagina. Tissue is taken from the front wall of the vagina for this purpose.
Diagnosis/Preparation
Diagnosis
The diagnosis of hypospadias in boys is often made at the time of delivery during the newborn examination. The condition may also be diagnosed before birth by ultrasound; according to a group of Israeli researchers, ultrasound images of severe hypospadias resemble the outline of a tulip flower. Ultrasound is also used prior to surgical repair to check for other abnormalities, as about 18% of boys with hypospadias also have cryptorchidism (undescended testicles), inguinal hernia, or defects of the upper urinary tract.
Hypospadias in girls may not be discovered for several months after birth because of the difficulty of examining the vagina in newborn females.
Preparation
Male infants with hypospadias should not be circumcised as the foreskin may be needed for tissue grafting during repair of the hypospadias.
Some surgeons prescribe small doses of male hormones to be given to the child in advance to increase the size of the penis and improve blood supply to the area. The child may also be given a mild sedative immediately before surgery to minimize memories of the procedure.
Aftercare
Short-term aftercare
Many anesthesiologists provide a penile nerve block to minimize the child's postoperative discomfort. Dressings are left in place for about four days. The surgeon places a stent, which is a short plastic tube held in place with temporary stitches, or a catheter to keep the urethra open. The patient is usually given a course of antibiotics to reduce the risk of infection until the dressings and the stent or catheter are removed, usually 10–14 days after surgery.
The child should be encouraged to drink plenty of fluids after returning home in order to maintain an adequate urinary output. Periodic follow-up tests of adequate urinary flow are typically scheduled for three weeks, three months, and 12 months after surgery.
Long-term aftercare
Boys who have had any type of hypospadias repair should be followed through adolescence to exclude the possibility of chronic inflammation or scarring of the urethra. In some cases, psychological counseling may also be necessary.
Risks
In addition to the risks of bleeding and infection that are common to all operations under general anesthesia, there are some risks specific to hypospadias repair:
- Wound dehiscence. Dehiscence means that the incision splits apart or reopens. It is treated by a follow-up operation.
- Bladder spasms. These are a reaction to the presence of a urinary catheter, and are treated by giving medications to relax the bladder muscles.
- Fistula formation. A fistula is an abnormal opening that forms between the reconstructed urethra and the skin. Most fistulae that form after hypospadias surgery close by themselves within a few months. The remainder can be closed surgically.
- Recurrent chordee. This complication requires another operation to remove excess fibrous tissue.
- Urethral stenosis. Narrowing of the urethral opening after surgery is treated by dilating the meatus with urethral probes.
Normal results
Hypospadias repair in both boys and girls has a high rate of long-term success. In almost all cases, the affected children are able to have normal sexual intercourse as adults, and almost all are able to have children.
Morbidity and mortality rates
Surgical repair of hypospadias has a fairly high short-term complication rate:
- leakage of urine from the area around the urethral meatus: 3–9%
- formation of a fistula: 0.6–23% for one-stage procedures; 2–37% for two-stage procedures
- urethral stenosis: 8.5%
- persistent chordee: less than 1%
Alternatives
There are no medical treatments for hypospadias as of 2003. The only alternative to surgery in childhood is postponement until the child is old enough to decide for himself (or herself) about genital surgery.
See also Orchiectomy .
Resources
books
"Congenital Anomalies: Chromosomal Abnormalities." Section 19, Chapter 261 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
"Congenital Anomalies: Renal and Genitourinary Defects." Section 19, Chapter 261 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
"Drugs in Pregnancy." Section 18, Chapter 249 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
"Infertility: Sperm Disorders." Section 18, Chapter 245 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
periodicals
Baskin, Laurence S. "Hypospadias, Anatomy, Embryology, and Reconstructive Techniques." Brazilian Journal of Urology 26 (November-December 2000): 621–629.
Fredell, L., et al. "Complex Segregation Analysis of Hypospadias." Human Genetics 111 (September 2002): 231–234.
Greenfield, S. P. "Two-Stage Repair for Proximal Hypospadias: A Reappraisal." Current Urology Reports 4 (April 2003): 151-155.
Hendren, W. H. "Construction of a Female Urethra Using the Vaginal Wall and a Buttock Flap: Experience with 40 Cases." Journal of Pediatric Surgery 33 (February 1998): 180–187.
Hughes, I. A., et al. "Reduced Birth Weight in Boys with Hypospadias: An Index of Androgen Dysfunction?" Archives of Disease in Childhood: Fetal and Neonatal Edition 87 (September 2002): F150–F151.
Klip, H., et al. "Hypospadias in Sons of Women Exposed to Diethylstilbestrol in Utero: A Cohort Study." Lancet 359 (March 30, 2002): 1102–1107.
Meizner, I., et al. "The 'Tulip Sign': A Sonographic Clue for In-Utero Diagnosis of Severe Hypospadias." Ultrasound in Obstetrics and Gynecology 19 (March 2002): 250–253.
organizations
American Academy of Pediatrics (AAP). 141 Northwest Point Boulevard, Elk Grove Village, IL 60007. (847) 434-4000. http://www.aap.org .
American Board of Urology (ABU). 2216 Ivy Road, Suite 210, Charlottesville, VA 22903. (434) 979-0059. http://www.abu.org .
American Urological Association (AUA). 1120 North Charles Street, Baltimore, MD 21201. (410) 727-1100. http://www.auanet.org .
Society for Pediatric Urology (SPU). C/o HealthInfo, 870 East Higgins Road, Suite 142, Schaumburg, IL 60173. http://www.spuonline.org .
other
Centers for Disease Control Press Release. Hypospadias Trends in Two U.S. Surveillance Systems [cited April 24, 2003]. http://www.cdc.gov/od/oc/media/pressrel/hypospad.htm .
Gatti, John M., Andrew Kirsch, and Howard M. Snyder III. "Hypospadias." eMedicine. January 31, 2003 [cited April 25, 2003]. http://www.emedicine.com/PED/topic1136.htm .
Santanelli, Fabio and Francesca R. Grippaudo. "Urogenital Reconstruction, Penile Hypospadias." eMedicine. November 6, 2002 [cited April 24, 2003]. http://www.emedicine.com/plastic/topic495.htm .
Silver, Richard I. "Recent Research Topics in Hypospadias." Society for Pediatric Urology Newsletter 1 (October 1999). http://www.kids-urology.com/HypospadiasResearch.html .
Rebecca Frey, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Surgery to correct hypospadias is done by a pediatric urologist, a surgeon with advanced training in urology as well as in treating disorders affecting children. According to the Society for Pediatric Urology (SPU), pediatric urologists educated in the United States have completed two years in a general surgery residency after medical school, followed by four years in a urologic surgery residency and an additional two years in a pediatric urology fellowship program.
Surgical procedures to correct mild or mild to moderate hypospadias with little chordee may be done on an outpatient basis. Correction of moderate or severe hypospadias with some chordee, however, involves hospitalizing the child for 1–2 days. Parents can usually arrange to stay overnight with their child.
QUESTIONS TO ASK THE DOCTOR
- How often do you perform hypospadias repair, and what is your success rate?
- How severe is my child's hypospadias, and what procedure do you recommend to correct it?
- What do you consider the best age for corrective genital surgery and why?
Coming always but sometimes after few seconds late. Guide me Plz?
please im seeking an assistance...
Tell me what to do.
Thanks: Chad
Please send me a list.
Where do I begin searching for the right surgeon? Should I contact a urologist and go from there?
Any replies will be appreciated.
Thank you, Don
thanks for your kind
We opted for surgery, thinking it was a relatively minor procedure. We were misinformed on several levels and it was a huge mistake.
#1 You must seek out a top pediactric urologist or two to get their assesement for your son. If he is good our experience is you might have to wait weeks for an appt.
#2 If you end up having surgery, get informed about catethers, BEFORE the surgery.
i) Insist on the pediactric urologist fastening the catether to you son's body after surgery. No, a nurse or other medical staff member is NOT sufficient to do this.
ii) Triple check the catether before you leave the hospital - that is is draining and it is properly fastened to prevent kinking or pulling on the body.
iii) Continously monitor that the catheder is draining. No drainage for a couple hours could very well indicate it is kinked / plugged which is a very serious condition. You MUST monitor this carefully.
iv) If the catheder becomes plugged, go to the emergency room ASAP. If you are unable to do this, carefullly remove all tape on the catheder so you can visibly see all lengths of the catheder, to verify there are NO kinks in the tube outside of the body.
v) While at any appointment, (ex dressing removal) or in the hospital, you must ASK questions about what any medical staff / nurse is ABOUT to do to your son. You must then give the OK. It is our experience many are unfamiliar with catheders and any dressing/tape applied to them. They can be EASILY accidentally cut by nurses/staff that are not paying attention.
#3 If the chordee repair fails, scar tissue can build in the urethra and it can basically become plugged, forcing surgery, to removing the problem urethra area which then creates a hypospadius condition.
#4 If you have a self created hypospadius condition due to situations like #3, it could take multiple surgeries to reconstruct the urethra.
many thanks